How do I ... perform closed reduction and splinting of a Distal Radius Fracture?

A 77 y/o female is out in her garden when her foot catches on some ivy and she falls on an outstretched right hand. She presents to your office or ER with complaints of right wrist pain and deformity. The pain radiates a little but she denies pain in the proximal forearm and elbow and in the hand as well.
You remember that we must order views of the exact injured area. So instead of getting forearm radiographs, you get dedicated wrist radiographs.
She comes back with 4 views of the right wrist. You remember that we determine our measurements based on the PA (posteroanterior) and Lateral views. The oblique views give a little information but that’s not where we determine the treatment plan.
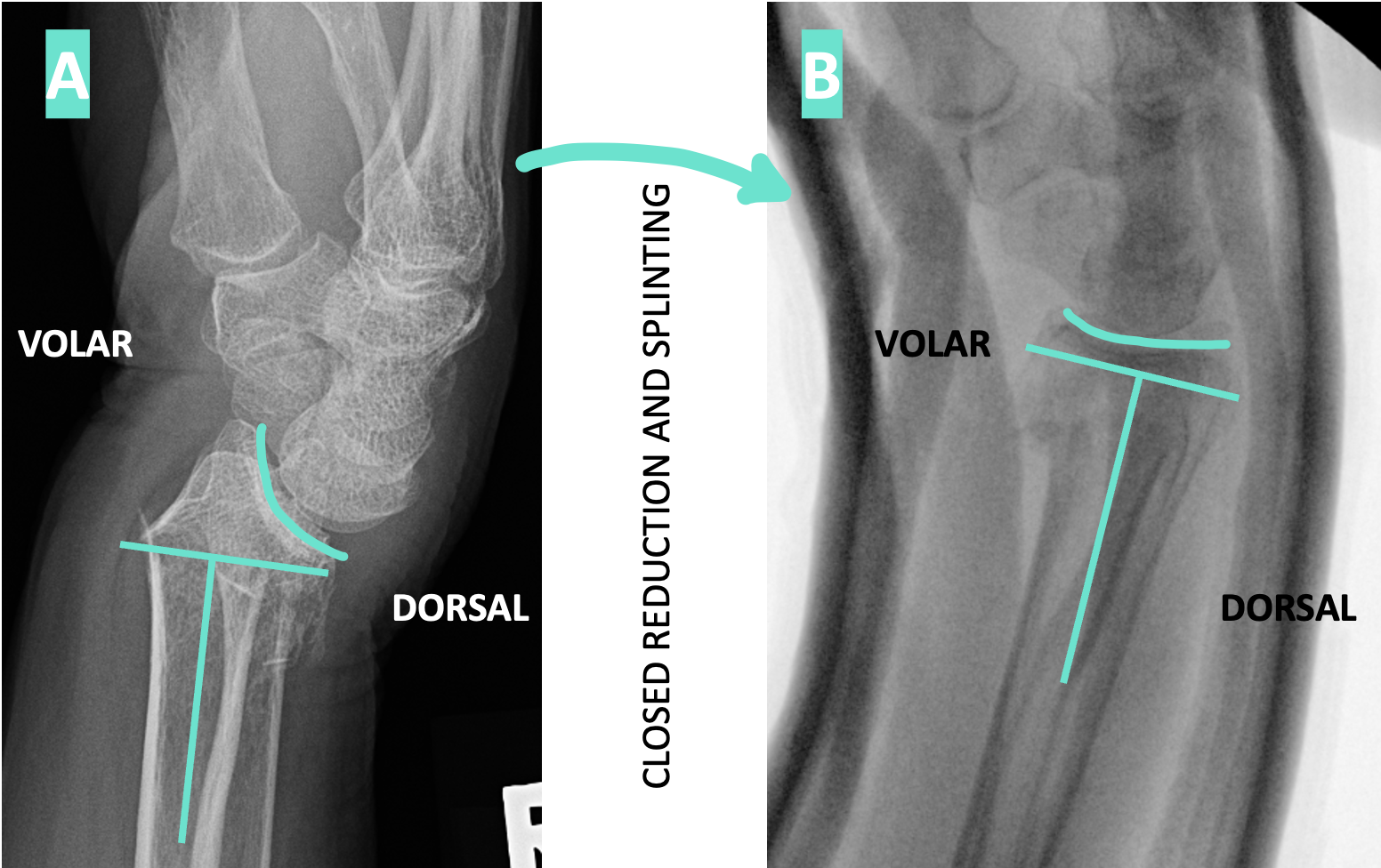
On the lateral view you determine which side is volar and which is dorsal. There is significant dorsal angulation - IT’S TIME FOR CLOSED REDUCTION AND SPLINTING! No need to ask for permission from ortho - you got this!
After providing a lidocaine hematoma block at the fracture site +/- sedation, the patient is placed in supine position and the arm abducted to 90 degrees. The fingers are then placed in fingertraps connected to an IV pole with counterweight over the humerus so the fracture is distracted for at least 5 minutes (this is called ligamentotaxis). (I do not personally have a YouTube video on this, but there are plenty out there ;-).
You perform a reduction technique on the distal radius1, apply padding starting at the distal palmar crease extending past the elbow with plenty of padding at the epicondyles and olecranon but not too much in the antecubital fossa. You then apply a SUGARTONG SPLINT (step-by-step instructions are here) with either fiberglass OneStep (measure and then cut) or plaster (measure your template, tear, then roll out 10 layers). You will need another set of hands usually ;-) Overwrap with elastic bandage.
As you mold the splint, avoid excessive wrist flexion as this can cause Median Nerve compression. Perform a complete post-reduction exam including sensation, motor and vascular exam.
→ All the while you have addressed the patient’s pain with medication and a cold pack in their armpit (it works wonders)!
Check out those post-reduction xrays! What an improvement!! The patient is referred to Ortho for follow up. The splint that you placed could stay on for 3 weeks until the fracture is healed enough to transition to a short arm cast.
BE SURE TO TELL THE PATIENT -
- Finger motion: You must move the fingers, make a fist, straighten them completely, spread apart, etc. Don’t just wiggle the fingers or they will get stiff! You could give them a handout to remember what to do every hour. (Download this patient education handout!)
- Multimodal pain management: besides prescribing an opioid for night time pain, you could recommend things like alternating Tylenol Arthritis and Aleve (it works way better than Ibuprofen and ES Tylenol), ice/cold pack in the armpit, keep the hand elevated as much as possible on 2-3 pillows when not up and walking around. (Download this patient education handout!)
- Sling: wear this when up and walking around, otherwise have it off. Encourage the patient to move the joints that are not injured, such as the shoulder by doing Pendulum swings with the splint in place.
Here’s to providing exceptional orthopedic care!
Cheers,
Vanessa
Reference:
- Miller MD, Hart JA, MacKnight JM. Essential Orthopaedics. 2nd ed. Elsevier; 2020:388-390.

